 Español
Español English
English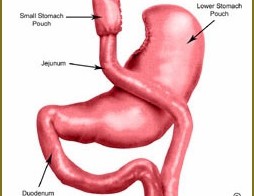
13
nov
2017
El presente vídeo expone de forma simplificada la realización de un Bypass gástrico... leer más
El presente vídeo expone de forma simplificada la realización de un Bypass gástrico... leer más

.. leer más
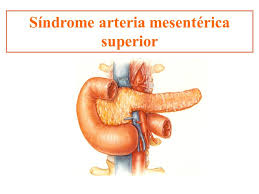
AIMS Wilkie’s syndrome is a rare condition (0.2%) that results from an intestinal obstruction due to compression of the third part of the duodenum between the abdominal aorta and superior mesenteric artery. Is most common in adolescents and young adults, especially women (2:1). Symptoms are nonspecific and may include postprandial epigastric pain, bloating, early satiety, nausea and vomiting. The pain is alleviated in the knee–chest position and in left lateral decubitus. CTA (Computed Tomography Angiography) and MRI (Magnetic Resonance Imaging) have shown greater sensitivity for diagnosis. Surgery is indicated if conservative management fails, in large evolution disease with significant weight loss and progressive duodenal dilatation or after complications such as peptic ulcer secondary to obstruction. METHODS We... leer más

AIMS Median arcuate ligament (MAL) syndrome is an uncommon condition caused by the external compression of the celiac trunk by the median arcuate ligament. MAL syndrome involves a constellation of symptoms including epigastric pain, postprandial pain, nausea, vomiting, and weight loss. Diagnosis is difficult and is made after exclusion of other more common causes of abdominal pain. Multiple imaging techniques can be used to demonstrate celiac artery compression by the MAL including mesenteric duplex ultrasonography, computed tomography angiography, magnetic resonance angiography, gastric tonometry, and mesenteric arteriography. Surgical options include isolated arcuate ligament chylotomy or associated angioplasty vs vascular reconstruction. METHODS We report the case of a 31-year-old man who presented epigastric abdominal pain and nausea without vomits for three... leer más

.. leer más
.. leer más

.. leer más

.. leer más
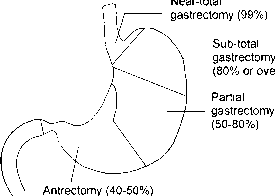
Presentamos un vídeo en el que mostramos una gastrectomía casi total (95%), en un paciente con un adenocarcinoma gástrico, con una anastomosis manual intracorpórea totalmente... leer más
La anastomosis esofagoyeyunal laparoscópica tras gastrectomía total constituye uno de los pasos más complejos de la gastrectomía laparoscópica, no sólo por la dificultad en su realización, sino también por el riesgo de dehiscencia de la anastomosis. Siguiendo las impresiones del Dr. Azagra, hemos intentado disminuir esta tasa de fístulas, así como facilitar la realización de esta compleja anastomosis, efectuando una gastrectomía casi total (95%), seguida de una reconstrucción gastroyeyunal siguiendo los mismos pasos que efectuamos en el by-pass gástrico. Nuestra experiencia inicial en 6 casos es bastante satisfactoria, con una tasa de dehiscencias del... leer más